Pick's disease is a rare, chronic and progressive disease of the central nervous system, characterized by atrophy of the temporal and frontal lobes of the cerebral cortex with increasing dementia.
The disease begins at 50-60 years of age, although there are later or earlier manifestations. Women tend to get sick more often than men. A. Pick in 1892 described cases of senile dementia, aggravated by the atrophic process mainly in the temporal and frontal lobes. Similar studies were carried out by A. Alzheimer, H. Lipman, E. Altman.
The statement that the cases of the disease described by A. Pick represent an independent form was first noted by H. Richter. This nosological independence of the disease was confirmed by pathological studies that showed a number of morphological features of this particular pathology.
Reasons for development
The etiology remains unclear. Family cases of the disease lead researchers to believe that it is hereditary. However, sporadic cases are observed much more often than familial ones, and within the same family, brothers and sisters are more likely to get sick than relatives in different generations. Possible etiofactors include long-term exposure to harmful chemicals on the brain.
This also includes the use of anesthesia, especially in cases of its frequent use or inadequate dosage. Some authors believe that Pick's disease may develop in connection with a previous mental disorder. Along with this, researchers are inclined to believe that factors such as intoxication, traumatic brain injury, infections, mental disorders, hypovitaminosis of vitamins c. They play only a provoking role.
Morphologically, atrophic processes are determined in the frontal and temporal lobes of the brain, often more pronounced in the dominant hemisphere. Atrophy affects both the cortex and subcortical structures. There are no inflammatory changes. Vascular disorders are not typical or mild. Senile plaques and neurofibrillary tangles typical of Alzheimer's disease are absent. Intraneuronal argentophilic inclusions are considered pathognomonic for Pick's disease.
Clinical picture
Studying the dynamics of these diseases with similar symptoms, doctors identified distinctive criteria for their differences:
- in PD, areas of neuronal damage and their atrophy are observed only in the frontal and temporal regions of the brain;
- protein plaques in vessels and neurofibers (unlike AD) are not observed;
- the death of neurons and thinning of the brain cortex in PD causes the disappearance of the boundaries between the white and gray matter of the brain;
- there is an increase in the ventricles of the brain;
- In PD, vascular pathologies in the brain are absent or insignificant.
The main sign of a rare, insufficiently studied and difficult to diagnose PD is obvious personality changes in a person. They are especially noticeable in the initial stage (at the age of 50 years). Later, increasing dementia is observed.
Frontal neuronal atrophy causes an unreasonable increase in mood, a careless attitude towards everyday and work problems, absent-mindedness, looseness and promiscuity (hypersexuality). Temporal – suspiciousness, obsessive feeling of inferiority, uselessness.
A person suffering from Pick's syndrome stops taking care of personal hygiene, and his vocabulary becomes impoverished. They may wander, leave home, and show sudden outbursts of aggression and agitation. At the same time, the ability to read, count, write, and intellectual functions (memory, orientation) do not change for a long time.
In Alzheimer's, memory loss first occurs, followed by cognitive impairment. And personality changes (including speech problems), loss of everyday skills, and a tendency to vagrancy appear in the later stages. AD manifests itself in old age over 60 and many years pass before total senile dementia (up to 10).
In the absence of serious chronic illnesses, the disease is not fatal; “turning into a vegetable” at the last stage is a long process. Old people with asthma cannot independently perform any household processes (wash, dress, eat) and require constant care. Weakness and lack of interest in life can lead to illness, which is dangerous due to the development of pneumonia, pulmonary edema, and coma.
These differences help doctors differentiate between Alzheimer's and Pick's disease. Confirmation of the diagnosis will require hardware examination.
Classification
There are three stages of development of Pick's disease, each of which is characterized by its own clinical picture and prognosis. It should be noted that the development of the disease at the last stage is already an irreversible pathological process and often provokes the development of concomitant somatic diseases.
The following stages of development of the disease are distinguished:
- first or initial - negative changes in human behavior are observed. Most often, this is a selfish orientation, irritation, aggression towards others;
- the second is the progression of the clinical picture of the first stage, a person’s intellectual abilities deteriorate, there is no logical thinking, the patient cannot cope with basic hygiene procedures on his own;
- profound dementia, the person requires constant care.
At the last stage of the disease, drug therapy no longer makes sense. In this case, the basis for improving the patient’s quality of life is nursing care.
Difference from Alzheimer's disease
Pick's disease and Alzheimer's disease have one thing in common: dementia. You can differentiate one disease from another by the following criteria:
- Age differences. Pick's disease develops around the age of fifty, while Alzheimer's disease goes largely undiagnosed until the age of sixty.
- Memory. In the first phases of Pick's disease, there are no attention deficits; a person can navigate the terrain and perform mathematical calculations. In the case of Alzheimer's disease, the main symptom will be a sharp decline in memory.
- Tendency to aggression towards relatives. Patients with Pika disorder, starting from the early stages of the disease, become prone to vagrancy and resist care from loved ones. In patients with Alzheimer's disease, such manifestations occur much later.
- A question of permissiveness. With Alzheimer's disease, no personality changes occur in the first stages, while with Pick's disease, pathological emancipation is revealed when the patient mindlessly obeys his physiological instincts.
- Speech disorders. The primary symptom of Pick's disease is a noticeable loss of vocabulary. With Alzheimer's, in the first stages there is no deterioration in speech, and the process occurs more slowly.
- Reading and writing. Patients with Alzheimer's disease almost immediately lose reading and writing skills, while people with Pick's disease do not lose these skills for a long time
Comparison of Parkinson's disease and Alzheimer's disease
These types of diseases affect different parts of the brain. In Alzheimer's, the cortex suffers. Therefore, all changes concern the cognitive sphere. And Parkinson's affects the motor sphere. Tremor appears, clarity and smoothness of kinetics are lost.
How does Alzheimer's disease differ from Parkinson's disease?
| Parkinson's | Alzheimer's | |
| Causes | Not installed | Not installed |
| Changes in the brain | Neuronal destruction, formation of Lewy bodies | Neuronal destruction, amyloid accumulation, formation of neurofibrillary tangles |
| Memory disorders | In the terminal stage of the disease | Starts at the initial stage |
| Thinking | Not changed | Mild disturbances, worsening towards the end of the disease |
| Neurological disorders | Tremor, muscle stiffness, postural instability | Minor pyramidal and extrapyramidal disorders are possible |
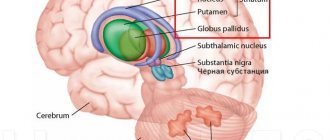
| Localization | Basal ganglia, substantia nigra (subcortex) | Cerebral cortex |
| Possibility of therapy and prevention | Regimen have been developed to treat symptoms. Surgical treatment is used in severe cases. | Symptomatic help and care |
Differences
The difference between Alzheimer's and Parkinson's is the nature of the disorders. In the first case, the patient is neurologically healthy. Only the patient’s psyche is subject to change. In the second case, the clinical picture is manifested by extrapyramidal disorders. Disturbances in gait, stride, tremor, and rigidity appear.
The psyche is destroyed again against the background of depression and apathy. The patient loses independence and usual ability to work. This becomes the cause of aggression and irritability.
Similarity
Parkinson's disease and Alzheimer's disease are degenerative diseases of the brain. Neurons die irrevocably, the possibility of their recovery has not been found. Maintenance therapy methods have been developed for pathologies. The drugs help control the symptoms of diseases.
Both diseases are classified as proteinopathies. With this pathology, the structure of the cell proteins changes, which leads to its death.
Diagnosis of Parkinson's and Alzheimer's
The approach to studying patients is no different from the previous case. It includes:
- Examination by a neurologist;
- Visualization;
- Laboratory tests;
- Functional tests;
- Psychiatric scales.
In Parkinson's disease, extrapyramidal disorders are detected. This is unsteadiness of gait, tremors, muscle tension. Such symptoms are rare in Alzheimer's dementia.
MRI in Parkinson's and Alzheimer's disease reveals cortical atrophy and ventricular enlargement. An accurate diagnosis can be made using PET or SPECT. Transcranial sonography is most often used in PD. The study reveals hyperechogenicity of the substantia nigra.
Functional tests include EEG. There are no distinctive features. Psychiatric testing detects dementia only in Alzheimer's disease. Dementia in Parkinson's develops in the later stages.
Difference in treatment
Alzheimer's dementia has no cure. Symptomatic medications relieve depression, apathy, and loss of independence. But dementia is not reversible. And with Parkinson’s pathology, therapy for many years preserves the patient’s ability to move, work and care for himself. Unfortunately, sooner or later the disease still wins.
Exercise is an important factor in PD. Exercise helps keep your muscles active for a long time. For Alzheimer's disease, exercises are only part of a complex of general strengthening gymnastics. Physical activity has little effect on the pathogenesis of the disease.
Survival prognosis for Alzheimer's and Parkinson's disease
Compared to 6-8 years with dementia, patients with Parkinson's disease are simply long-livers. The disease can last 10-20 years. At the same time, adequate treatment and exercise therapy help curb the further development of symptoms. Some Parkinson's patients live to a ripe old age.
Symptoms
In the initial stages of Pick's disease, patients experience the following symptoms: antisocial behavior, severe selfishness. They lose the ability to control their actions, as a result of which they become eccentric - in particular, they satisfy basic instincts, including sexual desire, regardless of the people around them and the situation. Criticism of one's actions is reduced. Against this background, various disorders are formed, such as bulimia or hypersexuality.
In the initial stages of Pick's disease, patients can be in a state of both euphoria and apathy. They develop a characteristic speech disorder, manifested in the constant repetition of the same anecdotes, phrases, individual words - the “gramophone record symptom.” As the disease progresses, sensorimotor aphasia develops - the ability to verbally express thoughts, as well as understanding the speech of others, is lost. Then other cognitive functions are lost: counting (acalculia), writing (agraphia) and reading (alexia).
Subsequently, patients lose the ability to consistently perform actions (praxis disorders), their perception of the world around them changes (agnosia), and memory loss occurs (amnesia). The outcome is profound dementia. Patients cannot care for themselves, are disoriented in time and space, and immobilized.
Stages of Pick's disease
A feature of this lesion of the cerebral cortex is a gradual increase in symptoms, which cannot be stopped. Development occurs from the degradation of social functions to physiological disorders, expressed in memory loss and the cessation of the ability to perform other tasks.
- At the first stage, a change in behavior is observed. A person may suddenly leave his job. Damage to the basal frontal lobes provokes activation of selfishness, disinhibition of desires, loss of criticism, sexual disinhibition, physiological needs can be coped with in an environment not intended for this. It is easy to identify lesions affecting the right hemisphere by the appearance of euphoria. When the right lobes are affected, the patient becomes depressed. In case of damage to convexial surfaces, leading to atrophy, the patient experiences emotional dullness. The death of other areas can provoke indifference, spontaneity and other atypical forms of behavior.
- At the second stage, focal symptoms increase, manifesting themselves in the form of agnosia. Patients have hearing and speech impairments, they lose tactile and visual perception. Due to moderate agnassia at this stage, complex motor acts begin to be disrupted. There is a gradual disintegration of speech from the use of stereotypical constructions when constructing phrases to the transition to echolalia. The patient can only repeat heard words and syllables. As symptoms increase in the second stage, the patient gradually ceases to clearly understand the purpose of using objects. For example, having received candy as a treat, the patient can unwrap it, throw away the sweet treat and start eating the wrapper.
- The third stage is accompanied by a transition to total dementia. The patient loses the ability to perform any conscious activity, the possibility of recognition disappears. The patient feels severe weakness, practically losing the ability to move independently. However, Pick's disease is not accompanied by paralysis. At the thermal stage of the third stage, the patient develops a vegetative coma.
All stages of the disease, with an unfavorable course, develop within 3-4 years. The use of modern drugs and techniques, the patient’s health status and other factors can extend the duration of the disease to 7-10 years.
In medical practice, the disease differs depending on the location of the affected areas:
- in the case of a predominance of atrophy in the frontal part of the brain, most patients suffer primarily from disorders responsible for storing memory;
- atrophy in the temporal lobe causes speech disorders of aphasia;
- when the hypothalamus is affected, patients lose the ability to concentrate, they suffer from psycho-emotional disorders, depression or euphoria.
In medical practice, differences are observed only in the early stages of the lesion. The listed symptoms are combined in cases of simultaneous damage to both lobes of the brain.
Pick's disease in children
Irreversible damage to the cerebral cortex, characteristic of Pick's disease, in most cases affects older people. But in exceptional situations, this complex diagnosis is observed in representatives of other age groups, including children.
The danger lies in family history. In the case of the presence of dementia caused by this diagnosis in relatives, in rare cases, Pick's disease can develop in children. Inheritance occurs according to an autosomal recessive principle. If the disease is diagnosed in one of the parents, the hereditary lesion can occur in a child of either sex. An unfavorable prognosis is given if the pathological gene is present in both parents.
The progression of the pathology occurs in the first weeks of life. At birth, the baby is considered completely healthy.
Manifestations of pathology include:
- the presence of constant nausea, which often leads to vomiting;
- the child has no appetite;
- liver size is increased;
- body weight is rapidly decreasing, the baby is significantly behind in growth compared to peers;
- lymph nodes enlarge;
- pigmentation is observed on the skin;
- The cornea of the eye becomes cloudy.
As a result of a significant increase in the size of the internal organs, the abdomen of a small patient appears disproportionately large.
Pick's disease is incurable regardless of the patient's age. As the child’s symptoms develop, the central nervous system becomes disrupted. This manifests itself in the absence of speech, “humming” in infants, and visual and hearing impairment is diagnosed. The baby may develop seizures, similar to manifestations of epilepsy. Reflex activity in patients increases significantly. In the most difficult cases, when the disease starts in the first months, children rarely survive to one year.
In addition to the classic form of Pick's disease, children may develop:
- visceral type, most often beginning in children aged 6-7 years;
- in adolescence, the juvenile type of Pick's disease begins;
- A special form of Novo Scottia, also most often beginning in the first 20 years.
These types may not be accompanied by neurological disorders. In the juvenile type, children and adolescents experience severe muscle weakness, which can lead to loss of motor activity.
The choice of treatment option for pathology directly depends on the type of disease. The classic type develops rapidly and is fatal within a maximum of five years. Patients with other types can live up to 30 years.
Prevention includes testing with a geneticist for families planning to conceive a child.
Diagnostics
If you have the above-described clinical picture, you should contact a psychiatrist and neurologist. Diagnosis of suspected Pick's disease involves the following:
- Based on a physical examination of the patient and a personal conversation, the doctor assesses the patient’s psycho-emotional state;
- CT and MRI - to assess the condition of the brain;
- electroencephalography.
Laboratory tests, in this case, do not provide any diagnostic value. In some cases, a biochemical blood test may be necessary.
It should be noted that this disease must be distinguished from the following:
- brain cancer;
- Alzheimer's disease;
- Huntington's chorea;
- mental disorders in diffuse type atherosclerosis.
Based on the examination results, the doctor can determine the degree of development of the pathological process and choose the most optimal tactics of maintenance therapy.
MRI
Treatment
To date, there is no general method for treating Pick's disease. All a doctor can do is prescribe medication to delay progressive changes and improve a person’s condition.
Cholinesterase inhibitors are used in the treatment of Pick's disease. These are drugs such as Amiridin, Rivastigmine (Exelon), Reminyl (Galantamine), Aricept, and Gliatilin. These medications for Pick's disease normalize the condition of patients at an early stage of the disease. A good effect is obtained from the long-term use (about 6 months) of NMDA blockers (Akatinolmemantine), as well as nootropic drugs (Phenotropil, Aminalon, Nootropil) and Cerebrolysin. Relief of productive psychotic symptoms is carried out with mild neuroleptics - Teralen, Teraligen, Clopixol, Chlorprothixene.
Patients with Pick's disease require constant psychological support. Patients are recommended to participate in special training to slow the progression of the disease. The forecast for the future is unfavorable. Six years after the onset of the disease, complete moral and mental decomposition of the personality sets in, marasmus and cachexia set in. The sick person becomes completely lost to society. The patient needs mandatory constant care or placement in a specialized psychiatric hospital.
Treatment of Pick's disease
There is currently no specific therapy for Pick's disease. Its development is being carried out by leading medical centers, but has not yet led to guaranteed success. In order to alleviate the health condition of patients, supportive therapy is used.
The basis of the course are:
- galantamine, donepezil, choline alfoscerate and other anticholinesterase pharmaceuticals;
- in case of aggressive behavior of the patient, antipsychotics are prescribed
- nootropics, such as piracetam, gamma-aminobutyric acids, memantine.
Psychotherapy can play a major role in the early stages of the disease. Classes with a psychologist allow the patient to accept the fact of the onset of an incurable pathology. Understanding the problem can help a patient with initial brain damage to control his behavior.
Sessions with a psychologist are also recommended for the patient’s relatives. They allow you to adjust your behavior towards a sick close relative. At the third stage, constant supervision by a specialist is recommended. This allows timely changes to be made to the course of maintenance therapy. The use of effective techniques even during the transition to a vegetative state makes the patient’s situation easier.
In the early stages of the disease, physiotherapy and walking are recommended. Such measures help maintain the patient’s motor activity and reduce the rate of muscle atrophy. Presence training, sensory room, and art therapy are used.
Forecast
The prognosis for life with dementia associated with Pick's disease is unfavorable. The disease is incurable, and therapy is aimed at reducing and eliminating symptoms. Since the pathology develops gradually, its presence remains unnoticeable for a long time. Patients seek medical help late. This leads to rapid progression of the disease and deterioration of the patient's condition. Patients diagnosed with Pica live from 6 to 10 years with good care and effective treatment.
Often patients with dementia pose a danger to themselves and are unable to care for themselves - prepare food, dress, bathe, do laundry, clean. Therefore, such patients require constant care and monitoring. At the third stage of the pathology, patients often become immobilized due to apraxia and are disoriented. This leads to complications - bedsores, wound infections, sepsis, pneumonia. Complications often lead to the death of the patient.
With good care, effective drug and non-drug treatment, and surrounding the patient with care and warmth, the progression of the disease can be slowed down, the cognitive functions of the brain can be partially restored and the quality of life of a patient with Pick's disease can be significantly improved.
Prevention
An accident happened. The man was a bright personality, an interesting conversationalist, and wrote books. Suddenly he turned into an ill-mannered psychopath, stopped writing, was not interested in anything, and became aggressive. It turns out that the man got sick. The disease affects cell bodies located in the cerebral cortex. this causes complete destruction and change in personality. Which is very sad.
In order to prevent such misfortunes from happening to your family, it is necessary to carry out certain prevention. The risks of developing this disease should be removed from life. Try not to let her into your home.
Include folates in your daily diet, such as sorrel, cabbage, white and black beans. This is how we prevent the development of atherosclerotic vascular diseases.
You should eat sea fish, which contains instant Omega-3 fats, and flaxseed oil, which contains Omega-6.
Provide nutrition and good blood supply to the brain. You need to lose weight, consume all dairy products: cottage cheese, kefir, milk, sour cream, yogurt low-fat.
Try to learn something new. Learn languages, learn to play musical instruments. Any training and exercise should help the brain stay healthy. Dancing helps the brain work and create new chains of cells in the brain. Of course, with age, bones are already fragile, so they need to be strengthened and exercises done without sudden movements.