- October 18, 2018
- Psychological terms
- Liliya Chuyas
Each of us has psychological problems that interfere with our lives. The most effective way to get rid of them is cognitive behavioral therapy (CBT). How does the technique work, what are its features and when should it be used? The article will talk about how you can get rid of internal personal problems.
Cognitive Behavioral Psychology: Principles
CBT is a direction in psychology that originated in the 20th century. Today, methods and techniques of this type of therapy are constantly being improved.
A person makes mistakes in his life, and that's normal. However, “defeats” can affect later thoughts and behavior. Along with the situation, thoughts are born that predetermine the development of certain feelings. It is feelings that guide a person to one degree or another, after which a new situation appears, and so on in a circle.
For example, if a person convinces himself that he is powerless, incompetent, then in any difficult situation he becomes nervous and despairs. As a result, he does not make decisions and does not realize his desires. Because of such situations, neuroses arise and intrapersonal conflict occurs.
Cognitive behavioral therapy helps determine the source of difficult situations and a person’s depression. But most importantly, it helps to successfully combat these problems.
Goals of CBT in psychology:
- relieve a person from the symptoms of a neuropsychiatric disorder;
- minimize the likelihood of recurrence of neurosis;
- increase the effectiveness of medications prescribed by a doctor;
- eliminate stereotypes of behavior and attitudes;
- solve the problem of interpersonal interaction.
The essence of the cognitive approach is that all a person’s psychological problems are directly related to his thinking and beliefs. Intrapersonal conflict is the most common case of all current human problems. In this case, it is almost impossible to eliminate the problem yourself. Need help from a specialist.
What it is
Cognitive-behavioral therapy is a complex direction in psychotherapy, which is a collaboration of cognitive and behavioral (behavioral) approaches.
From the first, it has absorbed the postulates that all problems and disorders of the mental plane are caused by incorrect (illogical, inappropriate) beliefs, views, thoughts, life principles and priorities. They give rise to dysfunctional thinking patterns that lead to insoluble and difficult situations.
From behaviorism, CBT borrowed the idea that problematic, unhealthy, inappropriate human behavior is the result of improperly formed skills. But this can always be changed, based on the theory of conditioned reflexes of Academician Pavlov. Encouragement, reinforcement of desired patterns, lack of reward for mistakes and blunders - this is an effective tool for treating various types of mental disorders.
Cognitive-behavioral psychotherapy has absorbed the foundations of both directions and managed to harmoniously combine them into a single whole.
Cognitive behavioral therapy considers every problematic situation in the life of an ordinary person, as well as mental disorders and diseases, as a consequence of an incorrect pattern of behavior, which is based on a person’s negative thoughts and beliefs.
Let's consider the situation. The teenager is a member of an extremist youth group. Participates in the humiliation of persons of *** nationality on the territory of his city. He sincerely hates their representatives, is intolerant of their mere appearance, not to mention their statements and behavior. The root of evil is Nazi beliefs. The leaders of the organization treated the guy morally well, showing him only negative video materials about this nationality. First they anchored these thoughts in his head, and they already forced him to go out into the streets and act in this way.
The course of treatment in cognitive behavioral therapy always follows two directions: changing the way of thinking and behavior patterns. It is explained to the teenager that not all people of *** nationality are bad and he was shown only one side of the coin. He is introduced to the culture of their country, the most outstanding personalities, good deeds and actions of their representatives. Next, new patterns of behavior are reinforced (through role-playing situations, for example), encouraging the right choice and leaving without reward in case of an error.
The complexity of therapy is manifested not only in the harmonious combination of two directions. Its undoubted advantage is that it successfully solves both the personal problems of ordinary people (divorce, depression, self-doubt, complexes) and severe mental disorders (affective, intellectual-mnestic, organic, psychotic, emotional).
You can read about behavioral psychotherapy as a separate area in our previous article here.
Through the pages of history. Behaviorism became an independent movement in the 50s. XX century. A decade later, cognitive psychotherapy competed with it. In the early 80s. South African psychologist A. Lazarus, Canadian psychologist and psychotherapist D. Meichenbaum integrated both approaches in order to increase the effectiveness of each of them.
When should CBT not be used?
It is not recommended to use cognitive behavioral therapy if a person has mental disorders. This problem must be treated with medication and under the supervision of specialists.
Psychologists and psychotherapists cannot say unequivocally at what age one can start using cognitive behavioral therapy. It all depends on the specific situation and the methods that the doctor selects. Sessions are often conducted in childhood and adolescence.
Kinds
Each method is aimed at solving a specific situation and human problem. The specialist’s task is to get to the core of the problem and teach positive thinking techniques. Cognitive-behavioral methods:
- Cognitive therapy is used if a person perceives his life as a series of failures. The specialist must help the patient accept himself with all his strengths and weaknesses, as well as develop a positive perception of himself and his life.
- Reciprocal inhibition. If the patient has negative emotions and feelings, then during therapy they are replaced with positive ones. Anger is replaced by relaxation.
- Rational-emotional psychotherapy. The specialist helps the patient realize that thoughts are material. They must correspond to real life. And the fact that a person blames himself for unfulfilled dreams leads to neurosis and depression.
- Self-control. This technique is used if it is necessary to reduce a person’s outbursts of aggression.
- “Stop tap”, or control of increased anxiety. During the process of the technique, the person himself says “Enough!” yourself and your negative thoughts.
- Relaxation. The technique is used in conjunction with others to create a trusting atmosphere when working.
- Self-instruction. The essence of the technique is for a person to set tasks for himself and find ways to solve them.
- Self-observation is a technique that involves working with yourself. Keeping a personal diary is an effective way to track the source of problems.
- Analysis of consequences. During the session, a person changes negative thoughts to more positive ones. Of course, expecting early changes for the better.
- Search for advantages and disadvantages. Together with a specialist, the patient analyzes the situation and the emotions that he experiences in it.
- Paradoxical intention. This technique was developed by the Austrian psychiatrist Viktor Frankl. The person is asked to live through the problematic situation again and do the opposite. For example, if a patient has insomnia, the doctor advises not to try to sleep, but to stay awake.
Gradually, a person stops thinking in a negative way about sleep, and the problem recedes.
When can cognitive psychotherapy help?
Cognitive psychotherapy is used in the correction of most mental and psychoemotional disorders. But most often this type of therapy is used to treat depression. A depressed person experiences an exaggerated sense of loss, which may be real or imaginary.
Depression is characterized by the presence of negative thoughts of several directions. First of all, the patient develops a negative image of himself; he considers himself a loser, an inferior person. At the same time, they are given a negative assessment of the world around them and passing events, as well as their own future. Experts call this the cognitive triad of depression. To overcome this psycho-emotional disorder, it is necessary to work in each of these directions, replacing dysfunctional thoughts with rational thinking.
In addition to treating unipolar depression and increased anxiety, this type of therapy is also used to eliminate obsessive-compulsive disorder, various phobias, eating disorders, migraines, anxiety and anger attacks, and other personality and behavioral disorders.
Cognitive methods can be part of complex therapy in the treatment of schizophrenia and bipolar affective disorder. The combination of psychotherapy with medication can eliminate hallucinations in patients with schizophrenia and mitigate other symptoms of this pathology. Researchers have proven its effectiveness in the correction of many somatic diseases.
During therapy, the therapist works to solve the problem; he does not change the patient's personality characteristics or shortcomings. From the very beginning, the patient and therapist must come to some kind of agreement, outline the range of problems on which they have to work. It is possible to eliminate the manifestations of the above-mentioned disorders with the help of experimental testing of disaptive thoughts.
Cognitive-behavioral techniques
Irrational thinking and emotions force a person to perceive reality in a slightly distorted form, in a negative light. As a result, a person loses control over himself and over and over again commits illogical actions, which he later regrets.
Cognitive behavioral therapy, exercises in particular, will help a person realize the unconstructiveness of his behavior.
Experts conditionally divide all cognitive techniques into four groups, which we will describe in detail below.
Principles, methods and techniques
Cognitive behavioral therapy (exercises and specific techniques will be discussed later in the article) is based on some postulates or principles that define key areas in working with clients:
- the principle of minimal intrusion - during therapy, specialists interfere in the patient’s personal life only to the extent necessary to correct his condition;
- “here and now” principle — the starting point of therapy is the problem that worries the person who has applied at that particular moment;
- the principle of the relativity of the concepts “disease-health” and “deviation-norm” - the psychotherapist does not impose his vision of normal and healthy behavior on the client, the goal of psychocorrectional therapy is the formation of optimal behavior for each specific patient;
- the principle of using the help of the patient’s loved ones (family or friends) - this is possible with the consent of all parties and has a positive effect on the motivation of patients, increasing their interest in a favorable outcome of therapy;
- the principle of the active and directive role of the psychotherapist - in CBT the technique of “talking out” problems and experiences is not used.
A specialist, as a rule, works according to a specifically developed plan and communication is built in such a way that the patient’s role is quite passive - he must answer questions and diligently carry out recommended practices.
To solve clients' problems, cognitive behavioral psychotherapy uses the following techniques and methods:
| Written recording of thoughts | The psychotherapist suggests writing down what exactly prevents you from performing this or that action. As a rule, this will be the first thought that you should focus on while working. |
| Distance technique | It consists in developing an objective attitude towards one’s own thoughts, when first comes the awareness of the automatism of the emerging thought-attitude, then the understanding that this thought brings fear, irritation, anger or other unpleasant emotions and, in the end, the client himself questions the truth of such false cognitions . |
| Keeping a journal to record thoughts | Helps to understand exactly what thoughts a person spends his time on, and which of them are toxic to his consciousness. |
| Special cognitive rehearsal | When, while working with a specialist, the patient consciously reproduces destructive thoughts in his imagination and describes to him his emotions and sensations. |
| Repressing negative emotions | This technique helps victims of various crimes and people who have suffered various traumatic situations, when, instead of constantly replaying the details of what happened in their head, a person sets himself not to live in the past, and not to drag this burden into the present and future, and lets go of these events. |
| Decentration and decatastrophization | It is used to combat various types of phobias and patients with anxiety disorders. |
| Obsessive repetition of correct settings | This is the practice of repeating positive instructions that are written down on paper and read over and over again, leading to increased self-efficacy. |
| Channeling imagination in the right direction | For some patients, discomfort is caused not only by emerging events from the past and some incorrect attitudes, but also by a wild imagination. In this case, you should direct the coercive mental force to block the negative fantasies being played out in your head. |
| Replacing roles | The patient is asked to imagine that he needs to comfort a person who has the same problems as him. |
First group: track and understand
- Recording your own thoughts. A person should record his thoughts throughout the day on a piece of paper before performing any action. It is important to write down thoughts in their order. This is what will help you clearly see the significance of a person’s motives when making a decision.
- Keep a personal diary. Experts suggest that the patient write down thoughts in a short, concise form in a diary for several days. This step will help identify what a person thinks about most, what exactly worries him.
- Move away from irrational thoughts. The point is for a person to be objective about his own thoughts. To do this, he needs to become an “observer”. Look at the situation from the outside. Cognitive behavioral therapy talks about this. You need to do the exercises yourself and follow three steps:
- realize and accept the fact that the unconstructive thought that is overwhelming now was formed earlier, under different circumstances; this thought is imposed by someone or something, but is not a person’s personal opinion;
- realize and accept that if you think in stereotypes, then it will be impossible to adapt normally to living conditions and develop;
- question the emerging thought, idea, since stereotypical thinking does not correspond to the prevailing conditions of real life.
Basic Concepts
Without a theoretical basis, cognitive psychotherapy could not exist as a separate direction. Therefore, there are a few key concepts you should know.
Cognitive structure is a worldview that has developed in the mind as a result of upbringing, character development, training, observation and reflection.
Schemas are thoughts and feelings, responses that arise to external events under the influence of a cognitive structure. They can be adaptive and maladaptive, idiosyncratic and universal.
Cognitive errors are distortions of cognitive structure. These include:
- arbitrary conclusions - conclusions not supported by facts;
- overgeneralization - conclusions drawn on the basis of a single situation and then extended to all others similar to it;
- selective abstraction - focusing attention on only one side of an event while ignoring the rest;
- exaggeration and understatement - exaggeration of the situation and self-hypnosis that one cannot cope with it on one’s own;
- personalization - a person’s belief that what is happening is directly related to him, although in reality this is not the case;
- dichotomy of thinking - a categorical, polar assessment of oneself and events, either in an extremely rosy or extremely negative way;
- obligation - excessive responsibility where it is not required;
- prediction - a person’s confidence that he sees everything one step ahead, although in fact this is not the case;
- telepathy - the misconception that a person can read the thoughts of others;
- labels - associating oneself or others with negative types and patterns.
Automatic thoughts (AM) - what flashes through the brain with lightning speed, does not have time for a person to speak out, but causes a strong emotion. Initially, they are formed under the influence of experience. For example, a student constantly tells himself during a session that if he doesn’t pass it, it will be a shame. And, if he fails some exam, this automatic thought flashes in his head, but not formalized in the form of words. She can cause hysterics. AMs are distinguished by such properties as involuntariness, conciseness, lack of control, transience, intrusiveness and stereotyping.
Cognitive topics - psychopathology.
Second group: challenge thoughts that are “destroying from within”
The second group of cognitive behavioral therapy aims to challenge existing irrational thoughts. The specialist suggests that the patient adopt the following techniques:
- Give arguments for and against stereotypical thoughts. A person must write a maladaptive thought on a piece of paper, then divide the paper into two columns. Accordingly, identify the arguments for and against. Analyze your thought and make notes in both columns. The patient should then re-read his notes every day. If you regularly do this exercise, then the arguments in favor will be fixed in a person’s mind. But the “wrong” ones are eliminated from the mind.
- Weigh “+” and “-”. The point of this exercise is not to analyze your unconstructive thoughts, but to consider possible solutions. For example, a woman makes a choice between whether to maintain her own safety by not having contact with the opposite sex, or to accept the probable risk in order to create a strong, happy family.
- Experiment. The technique involves performing a certain emotion through personal experience. For example, if a person does not know how society will react to his outburst of anger, then the specialist suggests doing it immediately, showing anger at the therapist.
- Return to the past. The point of the exercise is to have a frank conversation with a fictitious impartial witness to the events that took place. Most often, such events leave a “visible” mark on the human psyche. This exercise will help you understand the other person's motives.
- Use of authoritative sources of information. The specialist selects information in advance from scientific literature, facts, statistics and personal experience. For example, if a person is afraid to fly on an airplane, then a specialist talks about objective reports. Thus, disasters happen much more often on the roads than in the sky.
- Socrates' method. If the patient is convinced that he will die from a spider bite, but at the same time says that he was previously bitten by this insect, then the specialist points out the contradiction in his words.
- Role reversal. Exchange of roles between specialist and patient. The person must convince the therapist that their thoughts are irrational.
Gradually, the patient himself becomes convinced that his judgments are maladaptive.
Basics
Principles
- Individual conceptualization of each patient is a combination of ideas about a given mental disorder within the framework of cognitive behavioral therapy and information about how it exists in a particular person.
- Creation of a strong trusting alliance between specialist and patient. Cooperation between them.
- Result-oriented, extremely focused on problematic thoughts and patterns.
- Emphasis on the present.
- Continuing education: the patient learns to be a psychotherapist for himself.
- Time limits: 15 sessions maximum.
- The structure of each session. No improvisation.
- Self-monitoring, self-instructions, and self-reflection are an integral part of CBT.
- The main thing is a change in thoughts and mood, and after them, behavior will be adjusted.
Methods
Reciprocal inhibition
Negative, destructive thoughts and behavior patterns are replaced by positive and creative ones. A good cognitive behavioral therapist understands how important it is not only to eliminate the wrong elements, but also to fill the voids that are created.
Example. The parents convinced their teenage daughter that dreadlocks were not entirely appropriate for a 12-year-old girl to attend a school with a strict dress code for appearance. However, they could not offer her anything in return, and she, abandoning this hairstyle, became interested in piercings.
Using reciprocal inhibition, the psychotherapist, through trial and error, will offer the teenager alternative options that will appeal to her and at the same time be positive. This could be the acquisition of basic hairdressing skills and the creation of unique beautiful hairstyles. Or teenage make-up lessons. Or a passion for high fashion shows.
Rational-emotive method
A person must realize that all his thoughts and behavior must be consistent with a realistic dream that can be achieved. For example, why smoke? Yes, it allows you to achieve momentary pleasure and calm down. But in the long term, these are yellow teeth, bad breath, lung diseases, which may include cancer. It is much healthier to acquire another habit - running in the morning. In the future, this will allow you to look young and feel good.
Using the rational-emotive method, the psychotherapist also explains to the patient that unrealistic dreams are the main source of depression and neuroses, so they need to be corrected in a timely manner.
Self-control
As part of cognitive behavioral therapy, a person learns to control his emotions and behavior in difficult, provoking situations. The main thing is to understand in time that this moment has arrived and the unconscious is taking over. At first, not everyone succeeds in this, but by performing certain exercises in classes with a psychotherapist, people acquire the ability to stop their own outbursts of aggression and other inappropriate reactions.
Emergency brake
Many people confuse this technique with the previous one. But this is not the same thing at all. Here the therapist works with the patient so that he can say “stop” to negative thoughts in a state of rest, and not in a stressful situation. Many people know when you can’t sleep because of obsessive ideas. They oppress, destroy internal harmony, and lead to the emergence of many complexes. The specialist creates in the person’s head an image of a bright red button on which is written in large letters: “Stop tap.” At such moments, you just need to press on it and switch to more positive thoughts.
Relaxation
This is a universal technique that is used in almost all areas of psychotherapy to establish a trusting relationship between the psychotherapist and his client. In this way, the specialist gains access to a person’s true thoughts, which are sometimes carefully hidden.
Self-instruction
When, during the sessions, destructive thoughts are clarified and a fight is waged against them, the specialist, together with his patient, develop clear instructions that must be strictly followed when a problematic situation arises.
Introspection
Psychotherapists use this method when a person refuses to acknowledge the destructive impact of his thoughts and behavior on his own personality and others. In this case, he is asked to keep a diary in which only facts are recorded. When a person re-reads them after a while and analyzes them, he independently comes to the conclusion that he should change something in his life.
Advantages and disadvantages
Often psychological problems are caused by the fact that a person sees only one side of what is happening. For example, a woman whose husband is constantly cheating puts up with him and is afraid to divorce him, because she is convinced that this will only make things worse for her (the social status of a single mother, decreased income). But as soon as she writes down the advantages of such a prospect on a separate sheet of paper (freedom, the possibility of a new personal life, peace of mind, absence of humiliation), they turn out to be much more numerous than the disadvantages. Changing her beliefs, she comes to the realization that she needs to decide to make drastic changes.
Paradoxical intention
An interesting method developed by the Austrian psychiatrist W. Frankl specifically for cognitive behavioral therapy. The patient is asked to first thoroughly understand his thoughts and isolate what he fears most. After all, all our problems and disorders are fueled by fears. We don't want to go to work because we're afraid of making a mistake and angering our boss. We worry about interpersonal relationships because we are afraid of being rejected, etc.
After clearly realizing your phobia, which is interfering with your life, you need to play it out in real life. Ailurophobes should pick up and stroke a cat, brontophobes should listen to recordings of thunder, demophobes should go outside and get lost in the crowd. If a person does what he fears every day, the fear will eventually go away.
Technicians
The techniques described above provide the basic techniques for working with thoughts and behavior patterns:
- keeping a diary with daily recording of your thoughts and behavior;
- reframing;
- examples from art (cinema, music, literature);
- empiricism;
- changing roles (this is the main technique);
- positive imagination;
- recording the pros and cons of what is happening;
- analysis of consequences.
Cognitive-behavioral therapy, which is a complex direction, is free in the choice of methods and techniques when working with the patient. It uses basic tools from both cognitive and behavioral approaches. Alternating them with each other. It allows you to achieve efficiency where other concepts lack the potential to solve problem situations.
Third group: activation of imagination
This group of techniques is aimed at activating the sphere of imagination. People with increased anxiety are dominated by obsessive, far-fetched thoughts and ideas that exhaust them from the inside. To overcome destructive thoughts, experts have developed a list of special techniques.
- Termination method. When a patient has a negative obsessive image, he should loudly and confidently shout the command “Enough!” Such a command stops the appearance of a negative image.
- Repeat method. If a person repeatedly repeats positive attitudes towards life, then his way of thinking becomes more productive.
- Using metaphors. Activating the realm of imagination requires the use of instructive parables, quotes and other metaphorical philosophical statements.
This epic approach to solving the problem is more understandable.
Cognitive-behavioral psychotherapy
Cognitive psychotherapy is one of the areas of the modern cognitive-behavioral direction in psychotherapy. Cognitive therapy is a model of short-term, directive, structured, symptom-oriented strategy for enhancing self-exploration and changes in the cognitive structure of the self with confirmation of changes at the behavioral level. Beginning - 1950-60, creators - Aaron Beck, Albert Ellis, George Kelly. The cognitive-behavioral direction studies how a person perceives a situation and thinks, helps the person develop a more realistic view of what is happening and hence more appropriate behavior, and cognitive therapy helps the client cope with his problems.
The birth of cognitive psychotherapy was prepared by the development of psychological thought in various directions.
Experimental work in cognitive psychology, particularly Piaget's research, provided clear scientific principles that could be applied in practice. Even studies of animal behavior have shown that we must take into account their cognitive capabilities to understand how they learn.
In addition, there was an emerging understanding that behavior therapists were unknowingly tapping into the cognitive capabilities of their patients. Desensitization, for example, takes advantage of the patient's willingness and ability to imagine. Likewise, social skills training is not actually conditioning, but something more complex: patients learn not specific responses to stimuli, but a set of strategies necessary to cope with fearful situations. It became clear that using imagination, new ways of thinking and applying strategies involves cognitive processes.
It is no coincidence that cognitive therapy originated and began to develop intensively in the United States. If in Europe psychoanalysis was popular in its pessimism regarding human capabilities, then in the USA the behavioral approach and the rather optimal ideology of the “self-made-man” prevailed: a person who can make himself. There is no doubt that in addition to the “philosophy of optimism”, the impressive achievements of information theory and cybernetics, and somewhat later the integration by cognitivism of the achievements of psychobiology, “fed” the humanistic pathos of the emerging model of man. In contrast to the “psychoanalytic man” with his helplessness in the face of the powerful forces of the irrational and unconscious, the model of the “knowing man” was proclaimed, capable of predicting the future, controlling the present and not turning into a slave of his past.
In addition, the widespread popularity of this trend was facilitated by the belief in the positive changes that a person is able to achieve by restructuring his ways of thinking, thereby changing the subjective picture of the world. In this way, the idea of a “reasonable man” was strengthened - exploring the ways of his knowledge of the world, rebuilding them, creating new ideas about the world in which he is an active figure, and not a passive pawn.
Aaron Beck is one of the pioneers and recognized leaders of cognitive therapy. He received his M.D. degree from Yale University in 1946 and later became a professor of psychiatry at the University of Pennsylvania. A. Beck is the author of numerous publications (books and scientific articles), which detail both the fundamentals of the theory and practical recommendations for providing psychotherapeutic assistance for suicide attempts, a wide range of anxiety-phobic disorders and depression. His fundamental guidelines (Cognitive Therapy and the emotional disorders, Cognitive therapy of depression) were first published in 1967 and 1979. Accordingly, they have since been considered classic works and have been reprinted several times. One of the last works of A. Beck (1990) presented a cognitive approach to the treatment of personality disorders.
Albert Ellis, the author and creator of rational emotive therapy (RET), has been developing his approach since 1947, the same year he received his doctorate in clinical psychology from Columbia University (New York). There, in 1959, A. Ellis founded the Institute of Rational Emotive Therapy, of which he remains the executive director to this day. A. Ellis is the author of more than 500 articles and 60 books that reveal the possibilities of using rational-emotive therapy not only in an individual format, but also in sexual, marital and family psychotherapy (see, for example: The Practice of Rational-Emotive Therapy, 1973; Humanistic Psychotherapy: The Rational-Emotive approach, 1973; What is Rational-Emotive Therapy (RET), 1985, etc.).
A. Beck and A. Ellis began their professional practice with the use of psychoanalysis and psychoanalytic forms of therapy; Both, having experienced disappointment in this direction, directed their efforts towards creating a therapeutic system that could help clients in a shorter time and was more focused on the task of improving their personal and social adjustment through awareness and correction of maladaptive thought patterns. Unlike A. Beck, A. Ellis was more inclined to consider irrational beliefs not by themselves, but in close connection with the unconscious irrational attitudes of the individual, which he called beliefs.
Proponents of the cognitive-behavioral approach assumed that a person builds his behavior on the basis of his ideas about what is happening. How a person sees himself, people and life depends on his way of thinking, and his thinking depends on how a person is taught to think. When a person uses negative, unconstructive, or even simply erroneous, inadequate thinking, he has erroneous or ineffective ideas and hence erroneous or ineffective behavior and the resulting problems. In the cognitive-behavioral direction, a person is not treated, but taught better thinking, which gives a better life.
A. Beck wrote about this: “Human thoughts determine his emotions, emotions determine appropriate behavior, and behavior in turn shapes our place in the world around us.” In other words, thoughts shape the world around us. However, the reality that we imagine is very subjective and often has nothing in common with reality. Beck repeatedly said: “It’s not that the world is bad, but how often we see it that way.”
Sadness is triggered by a willingness to perceive, conceptualize, and interpret what is happening primarily in terms of loss, deprivation, or defeat. With depression, “normal” sadness will be transformed into an all-encompassing feeling of total loss or complete failure; the usual desire to prefer peace of mind will turn into a total avoidance of any emotions, up to a state of “emotional dullness” and emptiness. At the behavioral level, in this case, maladaptive reactions of refusal to move towards a goal and a complete refusal of any activity arise. Anxiety or anger are a response to the perception of a situation as threatening, and the coping strategy for anxiety-phobic disorders most often becomes avoidance or aggression towards the “aggressor” when the emotion of anger is activated.
One of the main ideas of cognitive therapy is that our feelings and behavior are determined by our thoughts, and almost directly. For example, a person who was at home alone in the evening heard a noise in the next room. If he thinks they are burglars, he might get scared and call the police. If she thinks that someone forgot to close the window, she will probably get angry at the person who left the window open and go to close the window. That is, the thought that evaluates the event determines emotions and actions. On the other hand, our thoughts are always one or another interpretation of what we see. Any interpretation presupposes some freedom, and if the client has made, say, a negative and problematic interpretation of what happened, then the therapist can offer him, on the contrary, a positive and more constructive interpretation.
Beck called unconstructive thoughts cognitive errors. These include, for example, distorted conclusions that clearly do not reflect reality, as well as exaggeration or downplaying of the significance of certain events, personalization (when a person ascribes to himself the significance of events to which, by and large, he has nothing to do) and overgeneralization (on Based on one minor failure, a person makes a global conclusion for the rest of his life).
Let us give more specific examples of such cognitive errors.
a) arbitrary conclusions - drawing conclusions in the absence of confirming factors or even in the presence of factors that contradict the conclusions (to paraphrase P. Watzlawick: “If you don’t like garlic, then you can’t love me!”);
b) overgeneralization - the derivation of general principles of behavior on the basis of one or several incidents and their widespread application to both relevant and inappropriate situations, for example, the qualification of an isolated and particular failure as a “total failure” in psychogenic impotence;
c) selective arbitrary generalizations, or selective abstraction - understanding what is happening based on taking details out of context while ignoring other, more significant information; selective focus on negative aspects of experience while ignoring positive ones. For example, patients with anxiety-phobic disorders in the stream of media messages “hear” mainly messages about disasters, global natural disasters or murders;
d) exaggeration or understatement - a distorted assessment of an event, understanding it as more or less important than it actually is. Thus, depressed patients tend to downplay their own successes and achievements, lower self-esteem, exaggerating “damages” and “losses.” Sometimes this feature is called “asymmetrical attribution of luck (failure), which implies a tendency to attribute responsibility for all failures to oneself, and to “write off” success due to random luck or a lucky break;
e) personalization - seeing events as the results of one’s own efforts in the absence of the latter in reality; the tendency to relate to oneself events that are not actually related to the subject (close to egocentric thinking); seeing in the words, statements or actions of other people criticism, insults addressed to oneself; with certain reservations, this includes the phenomenon of “magical thinking” - an exaggerated confidence in one’s involvement in any or especially “grand” events or accomplishments, faith in one’s own clairvoyance, etc.;
f) maximalism, dichotomous thinking, or “black and white” thinking - assigning an event to one of two poles, for example, absolutely good or absolutely bad events. As one of the patients we observed said: “From the fact that I love myself today, it does not follow that tomorrow I will not hate myself.” The phenomenon is closely related to the mechanism of defensive splitting; it indicates an unstable self-identity, its insufficient integration (“diffuse self-identity”). .
All of these examples of irrational thinking are areas of activity for a cognitive psychotherapist. Using various techniques, he instills in the client the skill of perceiving information in a different, positive light.
In summary, the general scheme used in cognitive therapy is:
External events (stimuli) → cognitive system → interpretation (thoughts) → feelings or behavior.
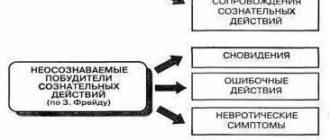
It is important that A. Beck distinguished between different types or levels of thinking. First, he identified voluntary thoughts: the most superficial, easily realized and controlled. Secondly, automatic thoughts. As a rule, these are stereotypes imposed on us in the process of growing up and upbringing. Automatic thoughts are distinguished by a kind of reflexivity, curtailment, conciseness, lack of control under conscious control, and transience. Subjectively, they are experienced as an indisputable reality, a truth that is not subject to verification or challenge, as A. Beck noted, like the words of parents heard by small and trusting children. And thirdly, basic schemas and cognitive beliefs, that is, the deep level of thinking that arises in the unconscious, which is most difficult to change. A person perceives all incoming information at one of these levels (or at all at once), analyzes, draws conclusions and builds his behavior on their basis.
Cognitive psychotherapy in Beck's version is structured training, experiment, mental and behavioral training designed to help the patient master the following operations:
- Discover your negative automatic thoughts
- Find connections between knowledge, affect and behavior
- Find facts for and against these automatic thoughts.
- Look for more realistic interpretations for them
- Learn to identify and change disorganizing beliefs that lead to distortion of skills and experience.
- Stopping technique: loud command “stop!” - the negative image of the imagination is destroyed.
- Repetition technique: we mentally scroll through the fantasy image many times - it is enriched with realistic ideas and more probable contents.
- Metaphors, parables, poems.
- Modifying imagination: the patient actively and gradually changes the image from negative to more neutral and even positive, thereby understanding the possibilities of his self-awareness and conscious control.
- Positive imagination: a negative image is replaced by a positive one and has a relaxing effect.
- negative view of the present: no matter what happens, a depressed person focuses on the negative aspects, although life provides some experiences that most people enjoy;
- hopelessness about the future: a depressed patient, picturing the future, sees only gloomy events in it;
- Decreased self-esteem: the depressed patient sees himself as inadequate, unworthy and helpless.
Stages of cognitive correction: 1) detection, recognition of automatic thoughts, 2) identification of the main cognitive theme, 3) recognition of generalized basic beliefs, 4) purposeful change of problematic basic premises to more constructive ones and 5) consolidation of constructive behavioral skills acquired during therapeutic sessions.
Aaron Beck and his co-authors have developed a whole range of techniques aimed at correcting automatic dysfunctional thoughts in depressed patients. For example, when working with patients who are prone to self-blame or taking on excessive responsibility, the reattribution technique is used. The essence of the technique is to, through an objective analysis of the situation, highlight all the factors that could influence the outcome of events. Having studied the fantasies, dreams and spontaneous statements of depressed patients, A. Beck and A. Ellis discovered three main themes as the content of basic schemes:
1) fixation on a real or imaginary loss - the death of loved ones, the collapse of love, loss of self-esteem;
2) a negative attitude towards oneself, towards the world around us, a negative pessimistic assessment of the future;
3) the tyranny of obligation, i.e. presenting strict imperatives to oneself, uncompromising demands such as “I should always be the very first” or “I should not allow myself any concessions”, “I should never ask anyone for anything” and etc.
Homework is of utmost importance in cognitive therapy. The undoubted advantage of cognitive psychotherapy is its cost-effectiveness. On average, a course of therapy includes 15 sessions: 1-3 weeks - 2 sessions per week, 4-12 weeks - one session per week.
Cognitive therapy is also highly effective. Its successful use leads to fewer relapses of depression than the use of drug therapy.
When starting therapy, the client and therapist must agree on what problem they will be working on. It is important that the task is precisely to solve problems, and not to change the patient’s personal characteristics or shortcomings.
Some principles of work between the therapist and the client were taken by A. Beck from humanistic psychotherapy, namely: the therapist should be empathic, natural, congruent, there should be no directiveness, client acceptance and Socratic dialogue are encouraged.
It is curious that over time these humanistic requirements were practically removed: it turned out that the straightforward-directive approach in many cases turned out to be more effective than the Platonic-dialogical one.
However, unlike humanistic psychology, which mainly worked with feelings, in the cognitive approach the therapist works only with the client’s way of thinking. In addressing the client's problems, the therapist has the following goals: to clarify or define problems, to help identify thoughts, images, and sensations, to explore the meaning of events for the client, and to evaluate the consequences of persisting maladaptive thoughts and behaviors.
Instead of confused thoughts and feelings, the client should have a clear picture. As the work progresses, the therapist teaches the client to think: turn to facts more often, evaluate probability, collect information and subject all this to testing.
Experienced testing is one of the most important points to which the client must be accustomed.
Hypothesis testing largely occurs outside the session, during homework. For example, a woman who assumed that her friend did not call her because she was angry called her to check whether her assumption was correct or not. Likewise, a man who thought that everyone was looking at him in a restaurant later dined there, in order to find that others were more occupied with their food and conversations with friends than with him. Finally, a freshman student, in a state of severe anxiety and depression, tried, using the method of paradoxical intention proposed by the therapist, to act contrary to her basic belief “If I can do something, I should do it” and chose not to strive for prestigious goals for which was initially oriented. This restored her sense of self-control and reduced her dysphoria.
If a client says, “When I walk down the street, everyone turns to look at me,” the therapist might suggest, “Try walking down the street and count how many people turn to look at you.” If the client completes this exercise, his opinion on this matter will change.
However, if the client’s belief was in some way beneficial to him, such an “objection” on the part of the therapist is unlikely to seriously work: the client simply will not perform the exercise proposed by the therapist and will remain with his previous belief.
One way or another, the client is offered different ways to test his automatic judgments with experience. Sometimes for this it is proposed to find arguments “for” and “against”; sometimes the therapist turns to his experience, to fiction and academic literature, and statistics. In some cases, the therapist allows himself to “convict” the client, pointing out logical errors and contradictions in his judgments.
In addition to experimental testing, the therapist uses other ways to replace automatic thoughts with thoughtful judgments. The most commonly used here are:
1. Revaluation technique: checking the probability of alternative causes of an event. Patients with depression or anxiety syndrome often blame themselves for what is happening and even for the occurrence of their syndromes (“I don’t think correctly, and that’s why I’m sick”). The patient has the opportunity to make his reactions more consistent with reality after reviewing the many factors influencing the situation or by applying logical analysis of the facts. A woman with anxiety disorder sadly explained that she felt nauseous, dizzy, agitated, and weak when she was “anxious.” After testing alternative explanations, she visited a doctor and learned that she was infected with an intestinal virus.
2. Decentration, or depersonologization of thinking, is used when working with patients who feel themselves in the center of attention of others and suffer from this, for example, with social phobia. Such patients are always confident in their own vulnerability to the opinions of others about them and are always inclined to expect negative assessments; they quickly begin to feel ridiculous, rejected, or suspected. The young man habitually thinks that people will think he is stupid if he does not appear completely confident in himself, on this basis he refuses to go to college. When the time came to submit documents to an educational institution, he conducted an experiment to reveal the actual degree of uncertainty. On the day of submitting documents, he asked several applicants like him about their well-being on the eve of the upcoming exams and the forecast for their own success. He reported that 100% of applicants were friendly towards him, and many, like him, experienced self-doubt. He also felt gratified that he could be of service to other applicants.
3. Conscious introspection. Depressed, anxious and other patients often think that their illness is controlled by higher levels of consciousness; constantly observing themselves, they understand that symptoms do not depend on anything, and attacks have a beginning and an end. Correcting the degree of anxiety helps the patient see that even during an attack, his fear has a beginning, a peak and an end. This knowledge allows one to maintain self-control, destroys the destructive idea that the worst is about to happen, and strengthens the patient in the idea that he can survive fear, that fear is short-lived and that one should simply wait out the wave of fear.
4. Decatastrophizing. For anxiety disorders. Therapist: “Let's see what would happen if...”, “How long will you experience such negative feelings?”, “What will happen then? You will die? Will the world collapse? Will this ruin your career? Will your loved ones abandon you? etc. The patient understands that everything has a time frame and the automatic thought “this horror will never end” disappears.
5. Purposeful repetition. Playing out the desired behavior, repeatedly trying out various positive instructions in practice, which leads to increased self-efficacy.
Working methods may vary depending on the type of patient's problems. For example, in anxious patients it is not so much “automatic thoughts” that predominate as “obsessive images”, that is, it is not thinking that is maladaptive, but imagination (fantasy). In this case, cognitive therapy uses the following methods to stop inappropriate fantasies:
One frequently used and very effective technique here is constructive imagination. The patient is asked to rank the expected event in “steps”. Thanks to acting out in the imagination and scaling, the forecast loses its globality, assessments become more gradual, and negative emotions become more accessible to self-control and manageable. In essence, the mechanism of desensitization is at work here: reducing sensitivity to disturbing experiences through calm and methodical comprehension of them.
In relation to depressed patients, cognitive therapists work based on their basic principle: a person’s feelings and states are determined by his thoughts. Depression occurs when a person begins to think that he is worthless or that no one loves him. If you make his thoughts more realistic and reasonable, then the person’s well-being improves and depression goes away. A. Beck, observing patients with neurotic depression, drew attention to the fact that themes of defeat, hopelessness and inadequacy constantly sounded in their experiences. According to his observations, depression develops in people who perceive the world in three negative categories:
To correct these problems, A. Beck compiled a behavioral therapeutic program that uses self-control, role-playing, modeling, homework and other forms of work.
J. Young and A. Beck (1984) point to two types of problems in therapy: difficulties in the therapist-patient relationship and incorrect application of techniques. Proponents of CT insist that only those with little understanding of cognitive therapy would view it as a technique-oriented approach and therefore fail to recognize the importance of the patient-therapist relationship. Although CT is a directive and fairly well-structured process, the therapist must remain flexible, willing to deviate from standards when necessary, adapting the methodological procedures to the individual patient.
Fourth group: minimizing resistance
Techniques from this group are aimed at increasing the effectiveness of the treatment process.
- Purposeful repetition. In personal practice, you need to persistently and repeatedly repeat positive attitudes. For example, when a person overestimates his own thoughts during sessions, he needs to effectively reinforce this exercise. The problem will no longer seem as global as the patient previously thought.
- Reveal hidden motives for destructive behavior. If a person continues to act illogically and think negatively for a long time, then the specialist’s task is to identify hidden motives.
Why does a person continue to behave this way? Is he comfortable living in a “box of negativity”? What's behind this? Finding secondary gain is a difficult task for a psychotherapist.
Aaron Beck
Aaron Beck is a famous psychotherapist from America who examined people with neurotic depression.
He concluded that depression and neurosis occur in people who:
- perceive everything that happens in a negative way;
- have powerlessness and hopelessness when making plans for the future;
- with low self-esteem and low self-esteem.
Beck's cognitive behavioral therapy was aimed at identifying a specific problem and how to solve it. At the same time, the psychotherapist did not correct the person’s personal qualities. His sessions were a series of questions and answers. Each question was asked so that the patient himself recognized the problem and understood where his destructive behavior and thinking could lead.
Aaron Beck's Cognitive Behavioral Therapy was a training program that could help you identify negative thoughts early, weigh the pros and cons, and then change your behavior pattern to produce a positive outcome.
Concept
Cognitive methods in psychotherapy work with the patient's thinking model .
The goal of cognitive therapy is awareness and correction of destructive patterns (mental schemes).
The result of treatment is complete or partial (at the patient’s request) personal and social adaptation of the person.
People, faced with unusual or painful events at different periods of their lives, often react negatively, creating tension in the body and brain centers responsible for receiving and processing information. This releases hormones into the blood that cause suffering and mental pain.
In the future, such a pattern of thinking is reinforced by repetition of situations, which leads to mental disorders. A person ceases to live in peace with himself and the world around him, creating his own hell .
Cognitive therapy teaches you to react more calmly and relaxed to inevitable changes in life, turning them into a positive direction with creative and calm thoughts.
The advantage of the method is working in the present tense, without focusing on:
- events in the past;
- influence of parents and other close people;
- feelings of guilt and regret about lost opportunities.
Cognitive therapy allows you to take your destiny into your own hands , freeing yourself from harmful addictions and the unwanted influence of others.
For successful treatment, it is advisable to combine this method with behavioral, that is, behavioral.
What is cognitive therapy and how does it work? Find out about it in the video:
What is a cognitive ability test for? Read about it here.
What happens during the session?
It is important to choose a specialist. He must have a permit to conduct activities and a diploma that confirms his qualifications.
Then a contract is concluded between the patient and the psychotherapist. It specifies key points, details of the session, its duration, number and conditions of meetings.
The contract must clearly state the basics of cognitive behavioral therapy, that is, the goal, and, if possible, the desired result.
There are two types of therapy courses:
- short-term – 15 sessions (duration – 1 hour);
- long – more than 40 sessions (1 hour each).
After meeting the patient and diagnosing his problem, the doctor must draw up an individual schedule for sessions. It is important to indicate the timing of meetings.
Education
Increasing the efficiency of your resources is important in any profession. Especially if this concerns practicing psychologists, psychiatrists and psychotherapists whose profile is cognitive behavioral therapy. Training will provide an opportunity to expand knowledge about the basic principles of this therapy. In addition, training will allow you to practice diagnostic tools in practice.
“Cognitive-behavioral therapy in Moscow” - special advanced training courses. This subject is mandatory in the training of European specialists. This program is adapted in Russia. Therefore, in addition to theory, it is possible to consolidate the acquired knowledge in practice. Training takes place on a paid basis.
There is a cognitive behavioral association. It was created in 1999 on the basis of the Neurosis Clinic named after. I. P. Pavlova. The Association of Cognitive Behavioral Psychotherapy is not state-owned, but has united more than 1000 specialists throughout Russia and abroad. Its founders are D. V. Kovpak, Yu. R. Palkin, A. V. Kurpatov, A. G. Kamenyukin and G. G. Averyanov.
By joining the association, participants can publish original articles on their personal profile on the website, propose topics for discussion, comment on other works of specialists, and maintain their own blog. The biggest benefit is being in contact with CBT practitioners. Also, members of the association take part in special events held by the association free of charge. Can participate in various professional conferences, forums, promotions, and seminars.
To join the Cognitive Behavioral Therapy Association, a member must:
- have a higher medical or psychological education (copies of diplomas - submit);
- know and practice in the field of psychology, psychotherapy, psychiatry, social work in the field of human mental health;
- voluntarily pay a membership fee.
You must fill out the form on the website.
Behavioral therapy
This therapy is designed to change inappropriate or ineffective behavior that is causing problems for the patient. Addictions, anxiety, phobias, and obsessive-compulsive disorder (OCD) respond well to behavioral therapy.
Behavior therapy is based on the following principle: because ineffective behavior is learned, it can be eliminated. There is no need to go into why and how this behavior occurs, the focus is on how to behave differently.
Thus, behavior therapy places less emphasis on past or childhood experiences and more on how current behavior and thoughts can be changed.
Behavior therapy is generally based on conditioning theory, and its various approaches are based on either classical or operant conditioning. (Classical conditioning produces involuntary, automatic behavior and stimuli, while operant conditioning uses reinforcement.)
The following types of psychotherapy are based on classical conditioning.
Systematic desensitization. The patient is gradually exposed to a fearful stimulus so that he gets rid of the conditioned response to it. For example, if a patient is afraid of spiders, he may first learn to talk or read about spiders without fear, then to be in the same room as a spider, then next to one, and eventually perhaps even to pick it up.
Psychological states. The therapist teaches the patient relaxation skills that can be used simultaneously with the feared stimulus, thereby reducing the conditioned fear response. This method has been successfully used to treat phobias and panic attacks.
Aversion therapy. Unlike systematic desensitization, which attempts to disrupt the connection between a stimulus and a negative response, aversion therapy attempts to create a connection when it is desired. For example, an OCD patient may tie a money band around their wrist when they have unwanted thoughts, thereby attempting to associate them with a (mildly) painful stimulus. When an alcoholic is given a drug with his consent that causes severe nausea when drinking alcohol, he learns to associate alcohol with unpleasant sensations, which leads to a decrease or cessation of alcohol consumption.
Immersion. The patient is “immersed” in his fear for a significant period of time until the high level of anxiety disappears. Theoretically, we cannot maintain a high level of arousal indefinitely. Eventually we will get tired and the anxiety will subside on its own. For example, a claustrophobic patient locked in an elevator will eventually stop worrying. However, there is one danger with this therapy: if the person refuses to continue the treatment (of course, patients can stop it whenever they want), the fear may even increase compared to what it was before the therapy.
Immersion must be used with caution: it can harm a person by forcing him to face his fears.
Therapies based on operant conditioning include the following.
Token reward system: As positive reinforcement, the patient is given “tokens” (points, stars, or stickers that can be exchanged for privileges, prizes, or other rewards) when he or she exhibits the desired behavior. This method is often used with people with learning difficulties to help them “shape” desired behavior by changing one aspect of it at a time, rather than changing the entire behavior. However, it can be used with anyone whose behavior we want to change, such as improving school attendance or reducing the number of times they are late to the office. But you need to make sure that the new behavior persists even after the reinforcement stops.
Modeling. Learning occurs through observation and imitation, and can be used as part of mentoring or buddying for children or people who have learning difficulties. The patient observes how someone else behaves correctly and copies him, learning the correct behavior. For example, a child who is afraid of dogs may watch his parents happily play with the dog and gradually realize that he has nothing to be afraid of.
Results
As you can see, the main task of a cognitive-behavioral specialist is not only to monitor the patient, but also to find out the origins of his emerging problems. It is important for a specialist to correctly explain to a person where the “legs” of all his failures “grow” from. Help him understand and accept the problem, build new positive behavioral attitudes towards life. For greater effectiveness, the patient must complete the “homework” given by the psychotherapist after the session. In addition, you can develop in this direction on your own so that cognitive-behavioral disorders never bother you again.
Coordinated work between both the specialist and the patient is important. Only in this case can the result be effective and improve the patient’s quality of life. Otherwise, only a person can influence the course of his thoughts. And a person’s life itself depends on what internal attitudes will be (positive or negative). His happiness is in his head!